
X
- No products in the list
Cystic Fibrosis (CF) is one of the most prevalent hereditary diseases with potentially fatal outcomes. In the Netherlands, approximately one in every 30 individuals is a carrier, resulting in one in every 3600 newborns diagnosed with CF. Around 1200 patients in the Netherlands live with this condition, and the median survival rate for CF patients hovers around 30 to 40 years.
The Genetics Behind Cystic Fibrosis
CF is an autosomal recessive disease caused by mutations in the ‘Cystic Fibrosis Transmembrane Conductance Regulator’ (CFTR) gene, situated on chromosome 7. The CFTR gene is responsible for the synthesis of the CFTR protein, a chloride channel. Dysfunction of the CFTR gene disrupts chloride transport in the epithelial cells of the lungs, respiratory system, sweat glands, pancreas, and reproductive organs, leading to severe chronic conditions like severe lung disease, salt depletion, pancreatic insufficiency, and infertility. The gene has over 2000 known mutations, and each influences protein function to some extent. Several hundred CFTR mutations have been proven to result in classic CF, with aberrant production or function of the CFTR gene if the mutations occur on both alleles.
Classifying CFTR Mutations and Their Impact
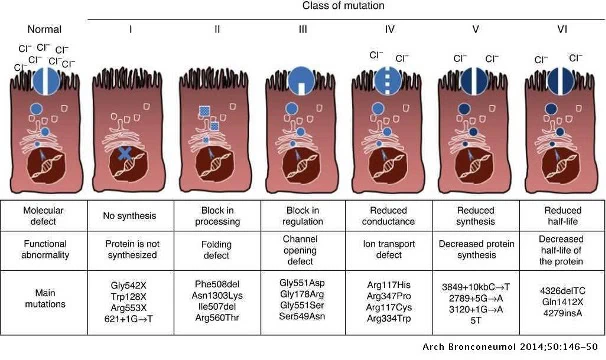
It is vital to categorize these mutations based on their effect on the CF protein to make informed therapy decisions. These mutations can be grouped into six classes. Class-I mutations (nonsense, frameshift, or splice mutations) produce truncated RNA, leading to the absence of CFTR protein at the apical membrane. Class-II mutations cause abnormal protein folding, resulting in degradation through a quality control mechanism. These mutations are most common in CF patients, with F508del being the most frequent.
Class-III mutations enable the CFTR protein to reach the membrane, but abnormal regulation of the chloride channel prevents proper opening. Class-IV mutations lead to reduced chloride conduction, resulting in a malformed CFTR pore with limited chloride ion flow. Class-V mutations result in reduced production of the CFTR gene, and the CFTR that is produced reaches the cell surface as normal.
Patients with Class IV and V mutations are generally diagnosed later in life, around 12 years of age, while those with Class I, II, or III mutations are diagnosed earlier, around 2-3 years. In the Netherlands, the A455E mutation (Class V) is the second most common after the F508del mutation.
Cystic Fibrosis: Incurable but Manageable
While CF is incurable, proper treatment can manage the symptoms. Therefore, early CF diagnosis is crucial. Early diagnosis can help prevent potential issues as much as possible. Patients diagnosed early exhibit almost similar growth and nutritional status as healthy children and maintain better lung function for longer. They also require fewer invasive treatments.
The ViennaLab CF StripAssays®: Enabling Early and Accurate Diagnosis
Establishing an early diagnosis is important, and this can be conveniently achieved through the ViennaLab CF StripAssays®. This reverse hybridization assay is tailored to population-specific mutations in various regions. The CF StripAssay® detects the 34 most common CFTR mutations, like F508del, and the IVS8 variants 5T/7T/9T. CF StripAssay®TUR and CF StripAssay®GER are also available, designed to detect the most common CFTR mutations in Turkish and German populations, respectively.
The StripAssay® is performed in three steps:
As of May 26, 2022, the new CD-IVDR regulation will be in effect within molecular diagnostics. This means that all molecular diagnostic tests must comply with the new regulations, and ‘home-brew’ kits will no longer be permitted unless there is no comparable commercial alternative available. Not all producers will comply with the new regulations for all tests, making certain tests like CF unavailable. However, nearly all tests from ViennaLab, including the CF StripAssays®, will comply with the new CE-IVDR regulations. For further information, please contact info@goffinmt.com.
References
[1] H. Heijerman, “Expressie van het cystische-fibrose-gen in de longen,” 2004.
[2] Nederlandse CF stichting, “CF: De basis – NCFS.” [Online]. Available: https://ncfs.nl/over-taaislijmziekte/cf-de-basis/. [Accessed: 22-Sep-2021].
[3] S. VEM et al., “Role of inflammation and oxidative stress in tissue damage associated with cystic fibrosis: CAPE as a future therapeutic strategy,” Mol. Cell. Biochem., Sep. 2021.
[4] M. Terzic, M. Jakimovska, S. Fustik, T. Jakovska, E. Sukarova-Stefanovska, and D. Plaseska-Karanfilska, “Cystic fibrosis mutation spectrum in north Macedonia: A step toward personalized therapy,” Balk. J. Med. Genet., vol. 22, no. 1, pp. 35–40, Aug. 2019.
[5] A. M. M. Vernooij-Van Langen, J. G. Loeber, C. P. B. Van Der Ploeg, E. Dompeling, and J. E. Dankert-Roelse, “Stand van zaken Neonatale screening op cystische fibrose in Nederland*.”
